Anna Zelencic Hayden DO, FACOFP, Allie Heineman OMS-III
This paper was submitted as part of Dr. Torrance's application for ACOFP Fellowship, which recognizes exceptional national, state, and local service through teaching, authorship, research, or professional leadership. Visit the ACOFP Fellows page to learn more about fellowship and the nomination process.
No disclosures to report
ABSTRACT
Background: Bone is the second most common site of thyroid cancer metastasis, after the lung. In most cases, thyroid carcinoma is found in thyroid tissue; reports of follicular thyroid carcinoma with a single metastasis to the ribs is rare, especially with no primary thyroid tumor found.
Case summary: This case report describes bone metastasis as the only clinical manifestation of thyroid cancer. The patient was a 77-year-old Jamaican woman with 2-year history of right shoulder pain radiating to right chest wall, breast region that was aggravated with deep inhalation and movement. In addition, the patient’s daughter later reported that her mother occasionally had a whistling sound coming from her chest. Five years prior, the patient had undergone left thyroid lobectomy with isthmectomy for aggressive thyroid goiter with tracheal compression. Prior to this procedure she underwent FNA aspiration biopsies that were indeterminate. On initial presentation, baseline chest x-ray and labs were obtained. Chest x-rays demonstrated focal opacity in the right upper lobe, new from the prior study. CT chest with contrast demonstrated expansile mass arising from the right 4th anterior rib. Primary differential diagnostic consideration was metastatic disease. CT guided biopsy of rib mass showed thyroid type cell proliferation containing colloid and forming follicular structures. Preoperative PET-CT studies were consistent with a lytic mildly hypermetabolic heterogenous expansile neoplastic mass of the anterior medial right 4th rib. A multidisciplinary collaboration and comprehensive treatment approach was adopted. The patient underwent complete thyroidectomy, total resection of the thyroid and right thoracotomy. There were no complications associated with the operation or its procedures and the patient had good postoperative recovery. The patient has since experienced no recurrence.
Conclusion: Follicular thyroid carcinoma is associated with early hematogenous metastasis, and the bone is a typical site of metastasis. Single bone metastasis is not a contraindication to surgical procedures and providing the appropriate therapy can result in better outcomes and quality of life for these patients.
THE CASE
A 77-year-old female presented as a new patient to establish care at a primary care physician’s office and obtain refills of her medications prior to travel. The patient was seen by another colleague within the health system in 2017-2018 and then transferred her medical care outside due to insurance concerns. Patient is retired and does mission work in Jamaica, so she travels quite a bit. She has a medical history of bilateral knee osteoarthritis, left shoulder osteoarthritis, hypertension, hyperlipidemia, type 2 diabetes mellitus and tinnitus. No pertinent social or family history. Past surgical history was significant including bilateral tubal ligation, appendectomy, hysteroscopy with dilation and curettage (benign findings) and most recently in 2017, left thyroid lobectomy with isthmectomy due to enlarged thyroid goiter with compressive symptoms including cough and painful swallowing. The preoperative fine-needle aspiration (FNA) thyroid biopsy was indeterminate. History showed she was refractory to aggressive medical management, so she underwent a CT scan with IV contrast which revealed large substernal goiter with airway compromise. The postoperative pathology report revealed multinodular goiter with colloid and hyperplastic changes.
On initial visit the patient complained of hoarseness since her partial left thyroidectomy 5 years prior and right shoulder pain that worsened over the last 2 years. The right shoulder pain radiated to right chest wall near the right breast region and was described as achy. Patient stated it worsened upon deep inhalation and movement. Patient reported pain was alleviated by rest and Tylenol. At the time of presentation, she was taking amlodipine, atorvastatin, and metformin. See her vitals in table 1.
| Table 1. Initial presentation vitals | |
| BMI | 41 kg/meters2 |
| Temperature | 97.6 F |
| Heart rate | 75 beats per minute |
| Respiration | 19 breaths per minute |
| Blood pressure | 165/72 mmHg |
Physical exam was essentially normal and musculoskeletal physical exam showed full range of motional bilaterally in the shoulders and a negative empty can test. Due to an elevated blood pressure at time of presentation, and vague chest wall discomfort, baseline electrocardiogram and chest x-ray, as well as monitoring labs for her chronic medical conditions, were ordered. An orthopedic referral was given to address her right shoulder pain. Patient received her travel medications.
Approximately 4 months after the initial visit, the patient returned to the USA and completed her previously ordered labs and x-rays. The chest x-ray showed a new right upper lobe focal opacity in comparison to her previous study in 2018, see image 1 and 2. Patient was seen in the office 3 days after her abnormal chest x-rays to follow up. During the visit she denied any shortness of breath with exertion. Her daughter then reported a whistle in patient’s throat. A subsequent chest CT scan was performed 19 days later which identified the opacity to be an expansile mass arising from the right 4th anterior rib. CT scan guided biopsy was performed of the right rib mass and pathology showed thyroid-type cell proliferation containing colloid and forming follicular structures. Immunoperoxidase stains showed that the cells are positive for transcription termination factor 1 (TTF1), and thyroglobulin and negative for Napsin A. The thyroid carcinoma NeoGenomics Molecular genetics profile study was negative for evidence of a fusion RNA alteration involving the genes on the panel.
PET-CT preoperative scan showed expansile lytic mildly hypermetabolic heterogenous neoplastic mass of the anterior medial right 4th rib. Labs had been drawn 4 months and 1 month prior to the surgery and day of surgery in which her alkaline phosphatase, liver function tests, and total bilirubin stayed within normal limits.
The patient then had a completion thyroidectomy and rib resection thoracotomy with 4th intercostal space mass total resection. Thyroid pathology showed benign thyroid tissue with colloid and hyperplastic changes, while the rib mass showed follicular thyroid carcinoma into the medullary bone and margins benign. The patient had an uncomplicated postoperative stay at the hospital and was discharged postoperative day 7. Since the patient had undergone completion thyroidectomy, hypothyroidism will always develop, and patients will require lifelong thyroxine replacement therapy.
During her one-month postoperative office visit the patient was referred for a PET-CT scan for restaging and endocrinology consultation. Results showed patchy uptake in right ribcage and chest wall likely due to postoperative uptake rather than residual or recurrent malignancy.
No evidence of distant metastases was noted, and close follow-up recommended was recommended. In addition, lab testing for her one-month status post completion thyroidectomy and right rib mass removal thyroid function was completed (see table 2).
| Table 2. One month post-surgery thyroid labs | ||
| Lab test | Result | Normal Range |
| Triiodothyronine | 21 (L) nanog/L | 71-180 |
| Thyroid Stimulating Hormone (TSH) | 22,200 mclU/ml (H) | 0.450-4.500 |
| T4 free | 0.15 nano/dl (L) | 0.82-1.77 |
| Thyroid antithyroid globulin Ab | <1.0* IU/ml | 0.0-0.9 |
| Thyroglobulin by IMA | 22.7*nanog/ml | 1.5-38.5 |
Postoperative PET-CT demonstrated changes to right ribcage and chest wall favored to be postoperative uptake rather than residual or recurrent malignancy. Patchy update in the right thyroid fossa appeared to be probably post treatment related.
The TNM staging system is used to classify differentiated thyroid carcinoma (Liu et al., 2017). Based on her age > 45years of age T0N0M1 stage IV. At this time of writing, our patient is still pending evaluation by oncologist.
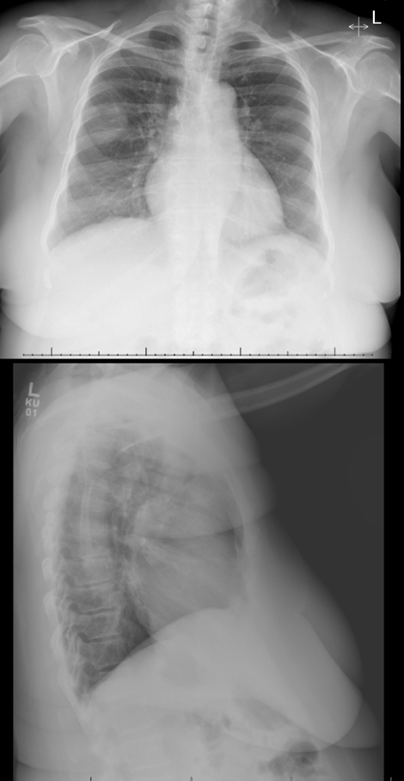
Image 1 & 2
DISCUSSION
Cancers that commonly metastasize to bone are breast, lung, thyroid, kidney, and prostate. Of note in this case no primary thyroid tumor was found in her thyroid.
Most follicular cancers present as solitary palpable nodules or enlarged thyroids. However, in some cases, the presenting sign is a pathologic fracture through a bony metastasis or a pulmonary lesion (Liu et al., 2017). Follicular thyroid cancers (FTC) make up 15-20% of thyroid tumors and are rarely fatal. Most patients are older than 40 and female (3:1). Bone metastasis from thyroid cancer, although less common than pulmonary metastasis, can significantly impact patient management and prognosis. The most common sites of thyroid cancer bone metastases are spine (34.6%), pelvis (25.5%), sternum and ribs (18.3%), extremities (10.2%), shoulder girdle (5.4%), and craniomaxillofacial (5.4%) (Osorio, et al., 2017). There is a controversy on whether iodine excess or deficiency causes thyroid cancer (Liu et al., 2017). Another source stated that the cause of thyroid cancer has links to several radiation exposure, iodine intake, diabetes, obesity, Hashimoto thyroiditis, exogenous estrogen use, and dietary choices (Aceves, et al., 2021).
Thyroid cancer typically follows an indolent course, with a relatively favorable prognosis but is one of the fastest growing cancers in the United States (Osorio, et al., 2017). However, in some cases, it can exhibit aggressive behavior, leading to distant metastases, most commonly lungs and bone. The case submitted here is of an elderly Jamaican woman with an unusual presentation of thyroid cancer, where bone metastasis was the only clinical manifestation.
Comparable to this case, Wexler, et al. (2011) presented a similar yet more advanced case of papillary thyroid carcinoma metastasizing to bone. In this case, proximal humerus, rib, vertebral body, and lung were involved. Another case had a 60-year-old female with distant thyroid cancer metastasis to her knee who solely presented with knee pain and a limp (Fataftah, et al., 2022).
The initial detection of the upper lung opacity on the chest x-ray emphasizes the importance of a comprehensive and thorough workup by the patient's osteopathic physician. In this case, the patient's presentation with essential hypertension and right chest wall pain led to a series of diagnostic evaluations that ultimately revealed the unexpected finding of the lung opacity to be a follicular thyroid carcinoma. Like this case and the other cases discussed it is paramount to keep the differential diagnosis open to help allow for early diagnosis and treatment to increase the likelihood of a favorable outcome.
CONCLUSION
Thyroid cancer is one of the fastest growing cancers in the United States as well as the most common endocrine cancer (Osorio, et al., 2017). As such it is exceedingly important to monitor patients with the standard of care post partial thyroidectomy. We present a case of metastatic thyroid cancer to the bone that despite its initial challenges and unexpected findings, ultimately lead to a promising outcome and long-term outcome for this patient. Follicular thyroid carcinoma often exhibits early hematogenous spread, frequently targeting the bones as a primary site for metastasis. It's important to note that the presence of a solitary bone metastasis should not deter consideration of surgical interventions. By implementing suitable therapeutic strategies, we can significantly enhance both patient outcomes and their overall quality of life. Overall, this case highlights a unique presentation of follicular thyroid cancer with bone metastasis as the sole clinical manifestation. This accentuates the importance of considering a diverse differential diagnosis to make a timely diagnosis and therefore treatment which will lead to a favorable outcome and improved quality of life.
REFERENCES
Aceves, C., Mendieta, I., Anguiano, B., & Delgado-González, E. (2021). Molecular iodine has extrathyroidal effects as an antioxidant, differentiator, and immunomodulator. International Journal of Molecular Sciences, 22(3), 1228. https://doi.org/10.3390/ijms22031228
Fataftah, J., Tayyem, R., Al-Dwairy, S., Al Manasra, A. R., Alawneh, K., & Al-Omari, M. (2022). Knee pain and limping as presenting symptoms of metastatic thyroid cancer. American Journal of Case Reports, 23. https://doi.org/10.12659/ajcr.938510
Liu, Y., Su, L., & Xiao, H. (2017). Review of factors related to the thyroid cancer epidemic. International Journal of Endocrinology, 2017, 1–9. https://doi.org/10.1155/2017/5308635
Osorio, M., Moubayed, S. P., Su, H., & Urken, M. L. (2017). Systematic review of site distribution of bone metastases in differentiated thyroid cancer. Head & Neck, 39(4), 812– 818. https://doi.org/10.1002/hed.24655
Wexler, J. A. (2011). Approach to the thyroid cancer patient with bone metastases. The Journal of Clinical Endocrinology & Metabolism, 96(8), 2296–2307. https://doi.org/10.1210/jc.2010-1996




